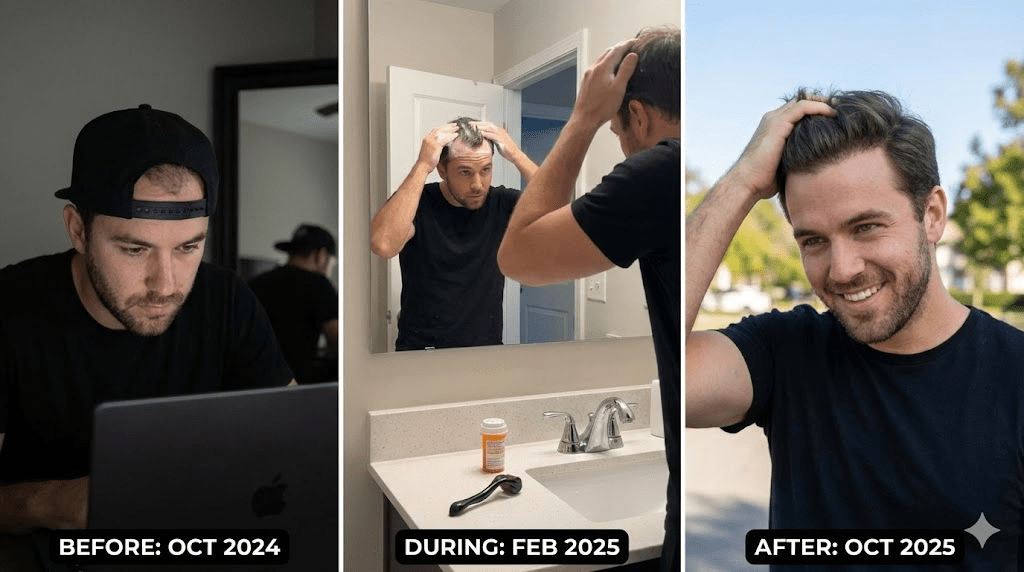
This guide breaks down "I Was the Guy in the Hat": How Alex Saved His Hairline (and His Confidence) Before 30 into the key mechanisms and the decisions that matter in practice. Alex, a 29-year-old software engineer, had a signature look: a black snapback cap. It wasn’t a style choice. It was camouflage.
“I wasn’t trying to look cool. I was trying to disappear.”
At 26, his shower drain started clogging. At 27, the “M” shape on his forehead became undeniable. By 29, he was comparing old photos of his father and realizing, with dread, that he was on the exact same timeline. Alex tried the usual consumer-route: thickening shampoos, biotin gummies, scalp brushes, caffeine serums. It felt like “doing something,” but the mirror kept moving in the wrong direction.
The moment the denial broke
The breaking point came at a friend’s outdoor wedding on a windy day. A gust pushed his hair back while the photographer was taking candid shots. When Alex saw the photos later, he didn’t see “a little thinning.” He saw a crown that was nearly see-through under natural light—the kind of lighting your bathroom never gives you.
The next morning he booked a dermatologist appointment. The diagnosis was quick and almost boring: Androgenetic Alopecia (male pattern hair loss). The doctor’s message was even more direct: this is not a shampoo problem. It’s a hormone-sensitivity problem.
The biology Alex was actually fighting
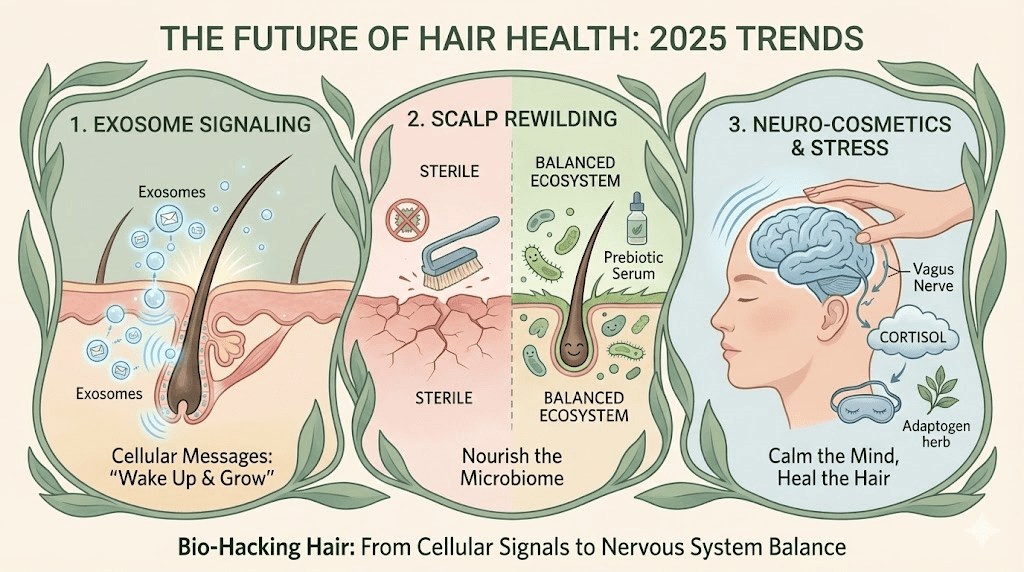
Most men think hair loss is “stress” or “bad genetics” in a vague way. The actual chain is more mechanical. Hair follicles on the scalp can be genetically sensitive to DHT (dihydrotestosterone). DHT binds to receptors in the follicle and gradually miniaturizes it—each cycle grows back thinner, shorter, and lighter until the follicle produces only peach-fuzz (vellus hair) or goes dormant.
- Key concept: You don’t “lose hair” overnight. You shrink follicles over years.
- Why the temples/crown first: Those follicles often have the highest genetic sensitivity to DHT.
- Why shampoo can’t fix it: Contact time is short; the mechanism is internal (enzyme + hormone + receptor).
The two decisions that matter most
Alex learned that hair loss outcomes are usually determined by two decisions—not by finding the “perfect product.”
- Decision #1: Start early. Saving miniaturizing follicles is easier than resurrecting fully dormant ones.
- Decision #2: Run a combined strategy. One tool slows the attack; another supports regrowth. Doing only one often leads to disappointment.
Baseline first: how Alex made it measurable
Before Alex started anything, his dermatologist insisted on a baseline. This is the part most people skip—and the reason they quit too early.
- Photos in consistent lighting: front, temples, top, crown (same distance, same bathroom, same time of day).
- Dermatoscope check: to confirm miniaturization patterns consistent with androgenetic alopecia (and not a different cause of shedding).
- A simple rule: no judging results before 12 weeks; no “success/failure” verdict before 9–12 months.
The protocol: what actually moved the needle
Alex committed to the evidence-based “stack” for a full year. Not because he loved routines—but because hair growth lives on a slow biological clock.
- The Shield: Finasteride (prescription, typically 1 mg daily)
Finasteride works upstream by inhibiting 5-alpha reductase, the enzyme that converts testosterone into DHT. In practical terms: it reduces the hormonal signal that’s shrinking the follicles. This is why it’s commonly described as “stopping the attack.”
- What Alex noticed: shedding slowed first (weeks to months), then stabilized.
- The mindset shift: finasteride is often more about preservation than dramatic regrowth.
- Safety note: side effects are possible for some men; work with a clinician rather than self-experimenting.
- The Fertilizer: Minoxidil (topical 5% foam or solution)
Minoxidil supports growth by improving follicle environment and prolonging the growth phase (anagen) for some hairs. It doesn’t address DHT directly—so on its own it can be a temporary win. Combined with a DHT blocker, it becomes far more strategic.
- Alex’s tweak: foam over liquid because his scalp got itchy.
- Consistency beats intensity: two minutes twice daily was easier than random “mega sessions.”
- Practical friction: he paired application with habits he already had (after brushing teeth).
- The Amplifier: Microneedling (clinician-guided or carefully at-home)
Microneedling can trigger a wound-healing cascade that increases local growth signaling and may improve topical absorption. For Alex, this was the lever that helped his temples—where he was most emotionally invested.
- Important precautions: sterile equipment, conservative frequency, and avoiding irritated/infected skin.
- Do not stack recklessly: many clinicians advise separating microneedling and minoxidil by a window to reduce irritation.
- If in doubt: have the technique demonstrated by a professional first.
The “Dread Shed” that almost made him quit
At around month two, Alex panicked: his shedding increased. It felt like proof he’d made everything worse.
“I was shedding more than ever. I thought I’d accelerated the end.”
His dermatologist explained the hair-cycle logic: many treatments push weaker hairs out of the resting phase so the follicle can re-enter a healthier growth cycle. The short-term shed is often the system “clearing inventory.” Not everyone experiences it, but when it happens, it’s psychologically brutal.
- What helped: having baseline photos, a timeline, and a clinician who normalized the process.
- What didn’t help: checking the crown under harsh overhead lights multiple times a day.
Timeline reality: what changed, and when
Alex stopped treating hair like a daily drama and started treating it like a long project with milestones.
- Month 3: shedding stabilized; fewer hairs on the pillow and in the drain.
- Month 4–5: early “peach fuzz” appeared at the temples; crown looked less “see-through” in daylight.
- Month 6–8: texture improved; hairs looked darker and stronger; styling became easier.
- Month 12: he could go hatless without feeling exposed.
Alex didn’t claim a perfect teenage hairline. What he got was something more valuable: control. He looked his age again—without hiding.
The support layer most men ignore
Alex also learned that while androgenetic alopecia is hormone-driven, outcomes are affected by the scalp environment and the body’s “construction materials.” This layer doesn’t replace the core protocol—but it can improve results and reduce irritation.
- Scalp inflammation control: gentle cleansing; avoiding harsh over-scrubbing; addressing dandruff if present.
- Fiber protection: minimizing friction, tight hats, and aggressive towel-drying.
- Nutrition basics: adequate protein; evaluating iron/ferritin and vitamin D if shedding is diffuse or sudden (with clinician guidance).
- Stress and sleep: not as a magical cure, but because chronic stress can add a telogen-effluvium overlay.
Common pitfalls (and why they backfire)
- Starting three new products at once and not knowing what caused irritation or what helped.
- Quitting at week six because “nothing happened” (hair biology is slow).
- Using unregulated “research chemicals” from the internet instead of clinician-backed options.
- Treating the strand while ignoring scalp inflammation and barrier damage.
Practical next steps
- Establish baseline photos and stick to a 9–12 month evaluation window.
- Reduce scalp irritation first: gentle cleansing and minimal harsh actives for 2–3 weeks.
- Choose one evidence-based intervention plan with a clinician (especially for prescription options) and commit.
- Protect hair fiber: minimize friction, heat, and prolonged wet time; use a microfiber towel.
Quick checklist
- Scalp is calm (less itch/burn).
- Routine is consistent for at least 8–12 weeks.
- Progress is measured with photos, not daily mirror panic.
- Heat and friction are minimized.
- Protein/iron status is considered if shedding is diffuse.